 |
|
|
|
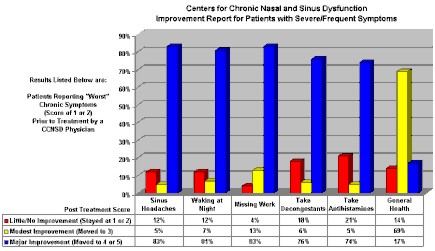
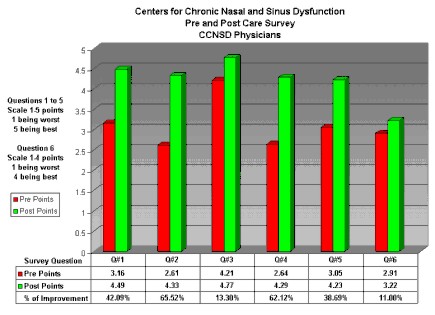
Pre and Post Care Survey
- All Patients
Question 1. After your treatment/ On a scale of 1 to 5, how would you describe sinus headaches? 1. Every day 2. Most Days 3.About half 4. Seldom 5. Never Question 2. After your treatment/ On a scale of 1 to 5, how would you describe waking up at night? 1. Every night 2. Most nights 3.About half 4. Seldom 5. Never Question 3. After your treatment/ On a scale of 1 to 5, how would you describe missing work or other activities? 1. All the time 2. Quite often 3.Sometimes 4. Seldom 5. Never Question 4. After your treatment/ On a scale of 1 to 5, how would you describe taking decongestants? 1. Every day 2. Most Days 3.About half 4. Seldom 5. Never Question 5. After your treatment/ On a scale of 1 to 5, how would you describe taking antihistamines? 1. Every day 2. Most Days 3.About half 4. Seldom 5. Never Question 6. After your treatment/ On a scale of 1 to 4, how would you describe your general health? 1.Poor 2. Fair
3.Good 4. Excellent *Review of Patient Health
Outcomes Report |